Melanoma
At QIMR there is a free tool, backed by evidence, with 70% accuracy of predicting that some one might develop melanoma over a 3 years period. Check it out here at: QIMR Berghofer Melanoma Risk Predictor Calculator:
https://publications.qimrberghofer.edu.au/Custom/QSkinMelanomaRisk)
The read all about melanoma here: www.melanoma.org.au
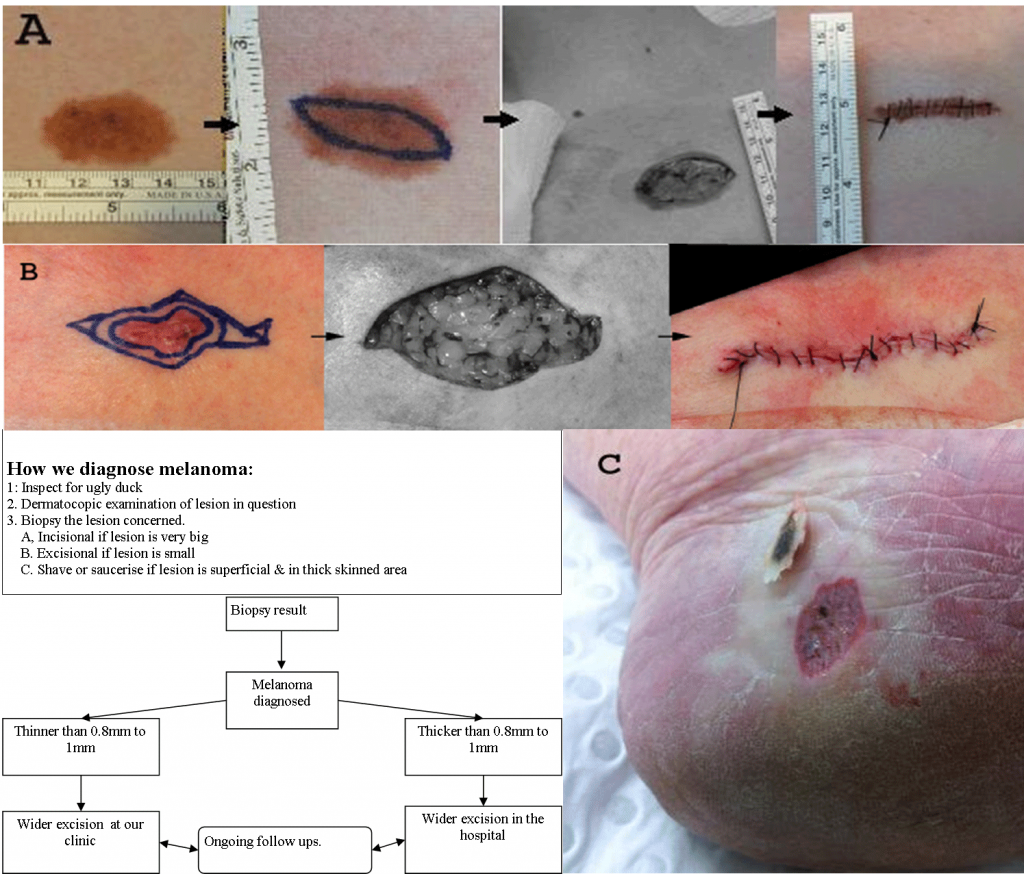
How we diagnose melanoma:
1: Inspect for ugly duckling
2. Dermatoscopic examination of any lesion in question
3. Biopsy the lesion concerned.
A, Incision if the lesion is very big
B. Excision if lesion is small
C. Shave or saucerise if lesion is superficial & in thick skinned area. Most doctors in general settings may see a few melanomas during their working life. At our clinics melanomas are commonly diagnosed. We see around 100 + melanomas per year. That’s a lot of melanomas. Fortunately, most are easily treated and the majority were treated at the clinic. A few patients were referred to the hospital for extra-attention.
In general dermatologists / skin cancer doctors do not operate on thick melanomas. Thick(~greater than 0.75-1mm thick ) melanomas are for the hospital surgeons. We normally refer patients to Wollongong surgical oncologist, Sydney melanoma unit or Westmead cancer care or Royal prince Alfred hospital . These centres are very efficient. If you have a melanoma > 1mm thick. You will be seen very quickly.










Excision of the melanoma site is easy. It’s the lymph node samplings and follow up care that really matter.
Melanoma – the dreaded skin cancer but, don’t panic! We have diagnosed and treated hundreds of melanomas over the years. Some of our patients have had multiple melanomas removed and are still in excellent health and living very normal lives. In general, we tend to see patients who are well motivated and who perform regular self skin checks, hence, the types of melanoma we see tend to be picked up in the very early stages. Early staged melanomas are easily picked with regular self examination.
Most melanomas illustrated here are fairly large >5mm and they look very sinister but, all these patients are a still well many years after diagnosis. It is not so much the size of the melanoma but, the THICKNESS of melanoma that determines your overall longevity and survival rate. For those unfortunate enough to have PINK melanomas and/or ( >0.8-1 mm in depth / thickness ) then we will facilitate speedy referral to a nearest melanoma unit on your behalf. Melanoma units are located at RPA hospital, Westmead hospital or in North Sydney ( next to the Sydney Adventist Hospital ).
In general dermatologists / skin cancer doctors do not operate on thick melanomas. Thick melanomas are for the hospital surgeons. We do of course do surgery on thick melanomas but only if the patient had an informed choice of whether he/she wanted lymph node biopsy or not. We also remove thick melanomas for palliation or patient requesting conservative treatments then office surgery will be sufficient. We do all these on a shared-cared basis with the hospital.
And remember: Melanomas do not appear over night. Generally if a mole has changed shape, size or colour over a 3 month period then you should have that mole examined in detail with dermatoscopy +/- biopsy ( incision or saucerisation NOT 2 mm punch biopsy ).See below for examples of melanomas looking with the naked eye and through a dermatoscope. Most are very obvious however, some are very normal looking. It takes experience to pick out early melanomas.
Some melanomas are just plain obvious, e.g. superficial spreading and pigmented nodular melanomas whilst some are just IMPOSSIBLE to diagnose by the naked eye e.g. pink or non pigmented or metastatic melanomas. The worse offender for delayed diagnoses will be the non-pigmented melanomas.